
What is a fibroid?
A uterine fibroid is also called a myoma of leiomyoma. It is a benign growth of muscle cells in the muscle layer of the uterus. A uterine fibroid can be on the outside of the uterus, in the uterine wall itself or in the uterine cavity. How a uterine fibroid is formed is not entirely known. A uterine fibroid can be a few millimeters, but also more than 10 centimeters.
A uterine fibroid occurs in about 70 percent of women, but causes complaints in about 25 percent. It is thought that growth occurs under the influence of female hormones. That is why a uterine fibroid never grows before the first menstruation. After menopause, uterine fibroids usually become smaller and the complaints less.
More often, uterine fibroids develop in women who do not (yet) have children and in women of African descent. A uterine fibroid usually does not cause any problems when becoming pregnant or during pregnancy, but can sometimes grow due to hormonal changes during pregnancy. After pregnancy, the uterine fibroids often become smaller again.

Example of multiple uterine fibroids (isala.nl)
What treatments are possible for a fibroid?
If you have no complaints, nothing needs to be done about uterine fibroids and no further control is necessary. If there are complaints, the woman chooses a treatment together with the gynecologist. The type of symptoms, the number , the location and size of the fibroids, your age, any desire to become pregnant and your preference for the type of treatment will all be taken into account. You can choose from several treatment options:
Medication
There is medical treatment with and without hormones. Medicines try to reduce the amount of blood loss and/or menstrual pain. The uterine fibroids remain; sometimes they get a little smaller. The effect of the medication depends on the amount, size and location of the uterine fibroid. After stopping the medication, the symptoms usually return.
isala.nl
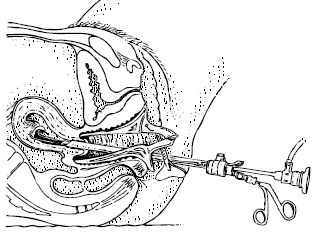
Hysteroscopy
In this procedure, the gynecologist removes a fibroid located in the uterus or bulging in the uterine cavity through the vagina. He or she will use a viewing tube. For this operation, you will be under anesthesia or receive an epidural.
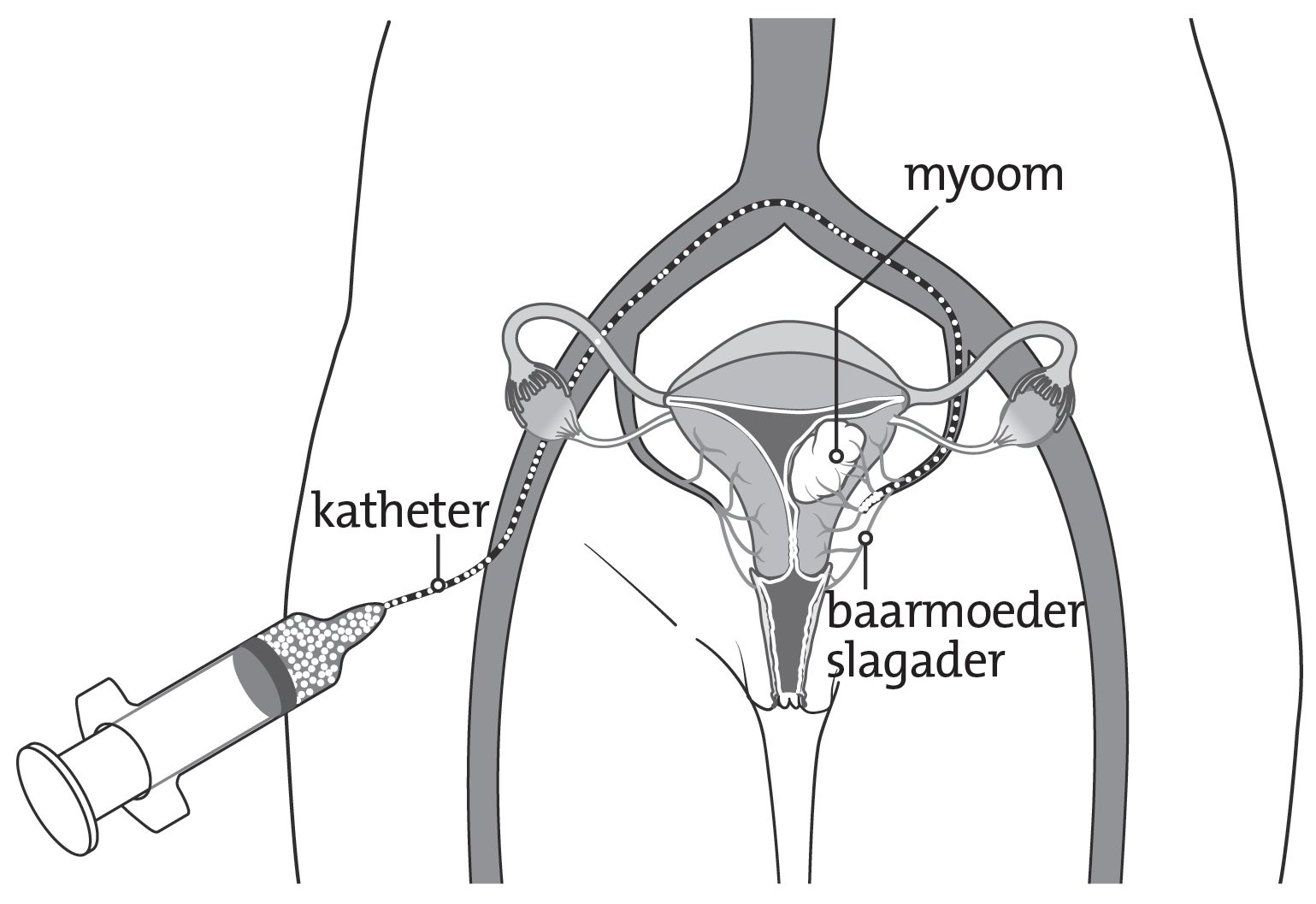
Embolization
isala.nl
During an embolization treatment, blood vessels leading to the fibroid are closed by filling them with small particles. These blood vessels are reached by moving a catheter via a vein of the groin all the way up to the uterine fibroids, which is all visualized by real-time angiography. Because the uterine fibroids now no longer receive blood, cell dead of the fibroid tissue will take place. Embolization is performed in the X-ray department by a radiologist.
Surgical removal of the fibroid (myomectomy)
If the fibroid is on the outside of the uterus or in the wall of the uterus, the gynecologist can surgically peel out the fibroid. This is called a surgical removal of a fibroid or myomectomy. A surgical removal of a fibroid can be done through laparoscopy or laparotomy. This treatment preserves the uterus itself. However, after fibroid surgery, adhesions may form in the cavity of the uterus, which may make it difficult to conceive. If the uterus is opened during the surgical removal of the fibroid, the gynecologist will recommend a C-section for future pregnancy.
Surgical removal of the uterus (hysterectomy)
Sometimes complete removal of the uterus is the best solution for the complaints. This is called surgical removal of the uterus or hysterectomy. This eliminates the blood loss; the effect on abdominal or back pain is less predictable. The uterus can sometimes be removed through the vagina, but in fibroids, this is usually done through the abdomen. This can be performed by means of laparoscopy or laparotomy. In principle, the ovaries and fallopian tubes remain in the abdomen. Fibroids cannot grow back after the uterus has been removed. Therefore, the surgical removal of the uterus is seen as the most definitive treatment.
MR-HIFU
MR-HIFU (Magnetic Resonance guided High Intensity Focused Ultrasound, a combination of MRI and ultrasound) is a relatively new treatment for women with uterine fibroids. The treatment started in 2009 at the University Medical Center Utrecht and at Isala women have been treated since 2016. Several thousand women worldwide have now undergone the treatment. This treatment is performed by the radiologist and takes place in day treatment. You do not need to stay overnight in the hospital after this treatment. More information can be found on the MR-HIFU page.
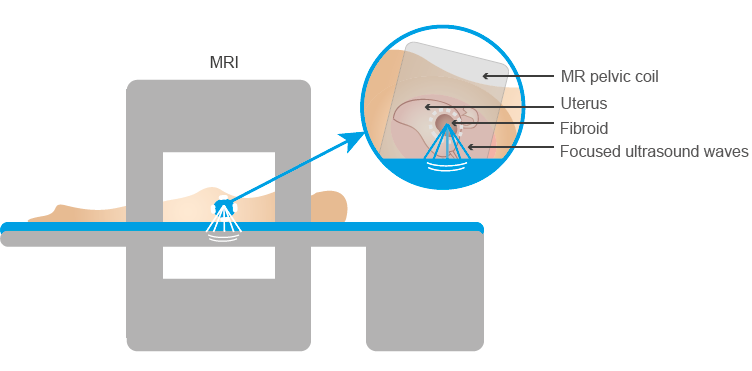
Position in MRI during MR-HIFU treatment for uterine fibroids (profoundmedical.com/sonalleve/)






